
E-Beta Thalassemia
Hb E/beta-thalassaemia: a common & clinically diverse disorder/RMCH.
Abstract
Haemoglobin E-beta thalassaemia (Hb E/β-thalassaemia) is the genotype responsible for approximately one-half of all severe beta-thalassaemia worldwide. The disorder is characterized by marked clinical variability, ranging from a mild and asymptomatic anaemia to a life-threatening disorder requiring transfusions from infancy. The phenotypic variability of Hb E/β-thalassaemia and the paucity of long-term clinical data, present challenges in providing definitive recommendations for the optimal management of patients. Genetic factors influencing the severity of this disorder include the type of beta-thalassaemia mutation, the co-inheritance of alpha-thalassaemia, and polymorphisms associated with increased production of foetal haemoglobin. Other factors, including a variable increase in serum erythropoietin in response to anaemia, previous or ongoing infection with malaria, previous splenectomy and other environmental influences, may be involved. The remarkable variation, and the instability, of the clinical phenotype of Hb E beta-thalassaemia suggests that careful tailoring of treatment is required for each patient, and that therapeutic approaches should be re-assessed over-time.
Keywords: Disease modifiers, genotype, haemoglobin E/β-thalassaemia, phenotye
Epidemiology
Worldwide, patients with haemoglobin E-beta-thalassaemia (Hb E/β-thalassaemia) represent approximately 50 per cent of those affected with severe beta thalassaemia1–7. The highest frequencies are observed in India, Bangladesh and throughout Southeast Asia, particularly in Thailand, Laos and Cambodia, where it is common for individuals to inherit alleles for both haemoglobin E (Hb E) and beta-thalassaemia6–8. Throughout these regions, Hb E/β-thalassaemia has become an increasingly severe public health problem. In Thailand, about 3,000 affected children are born annually, and estimates of about 100,000 living patients have been provided9. In southern China, due to gene frequencies of about 4 per cent for β-thalassaemia and for Hb E, thousands of patients are affected10. Hb E/β-thalassaemia is also common in Indonesia and Sri Lanka, and while previously rarely diagnosed in North America or Europe, has recently become the most common form of β-thalassaemia identified by many newborn screening programmes6,7,10–16.
There is a widely disparate range of clinical and haematological parameters in patients with Hb E/β-thalassaemia8,16–28. Its phenotypic variability, an emerging awareness that its phenotype may evolve over time, and the limited understanding of its natural history, combine to make the management of Hb E/β-thalassaemia particularly challenging29.
Pathophysiology
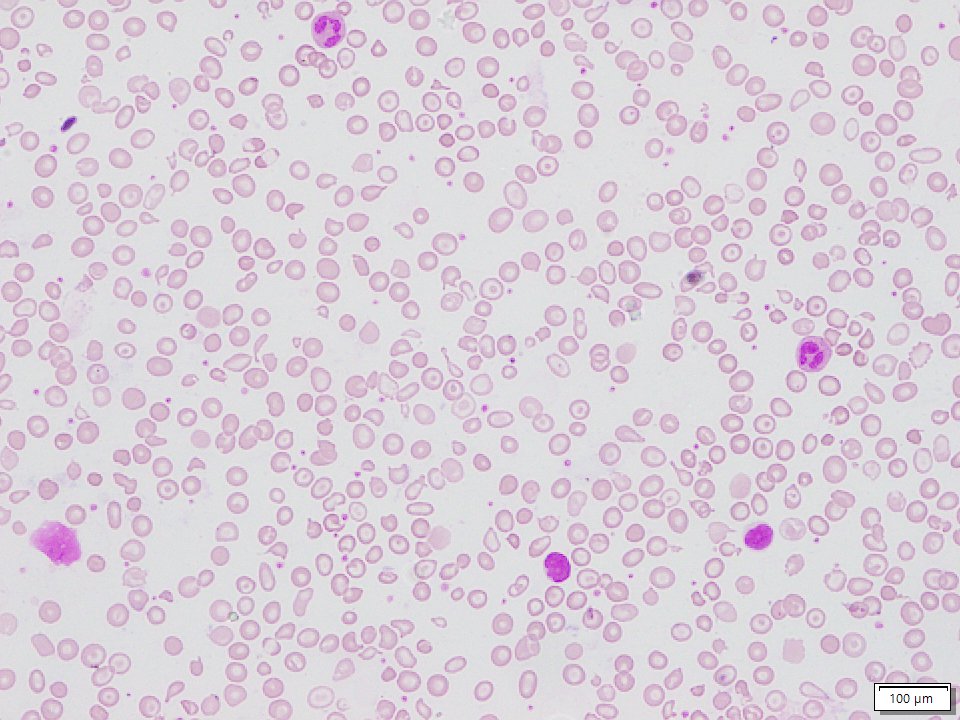
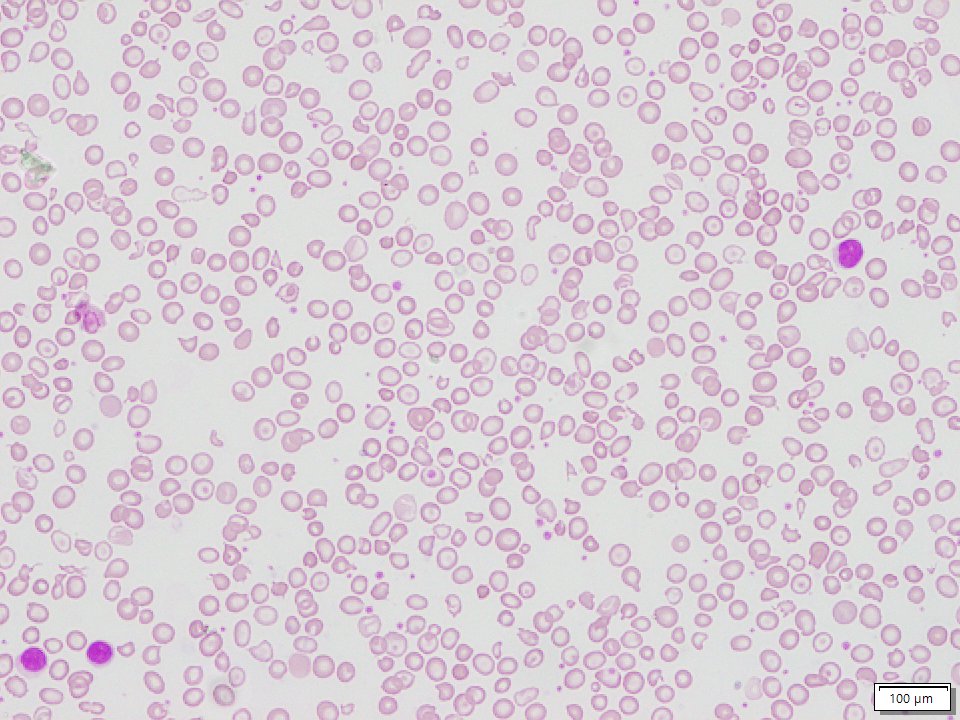
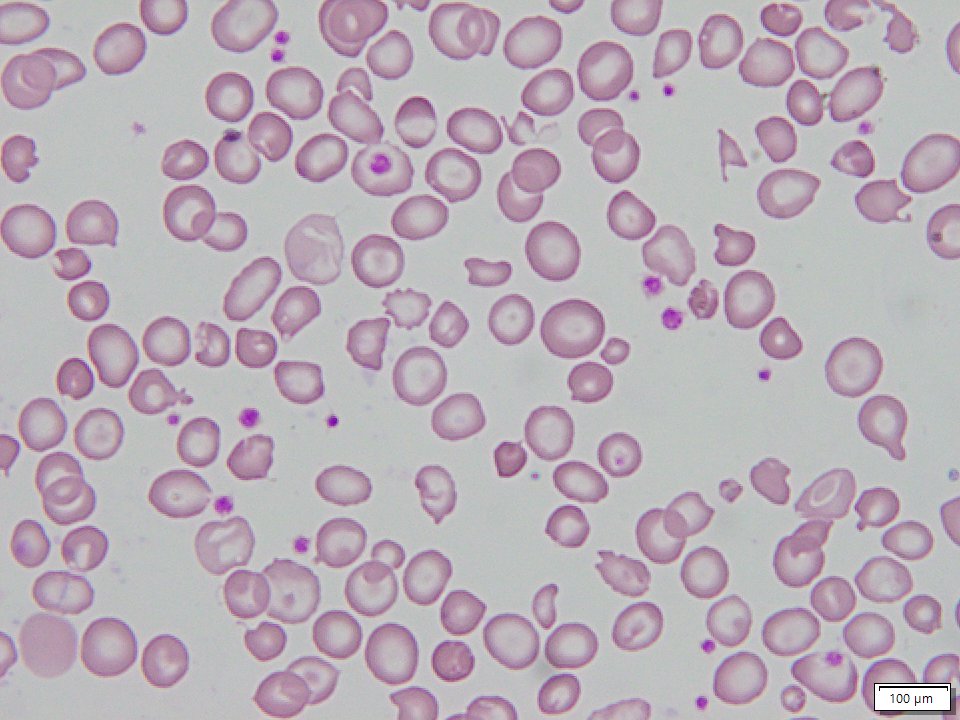
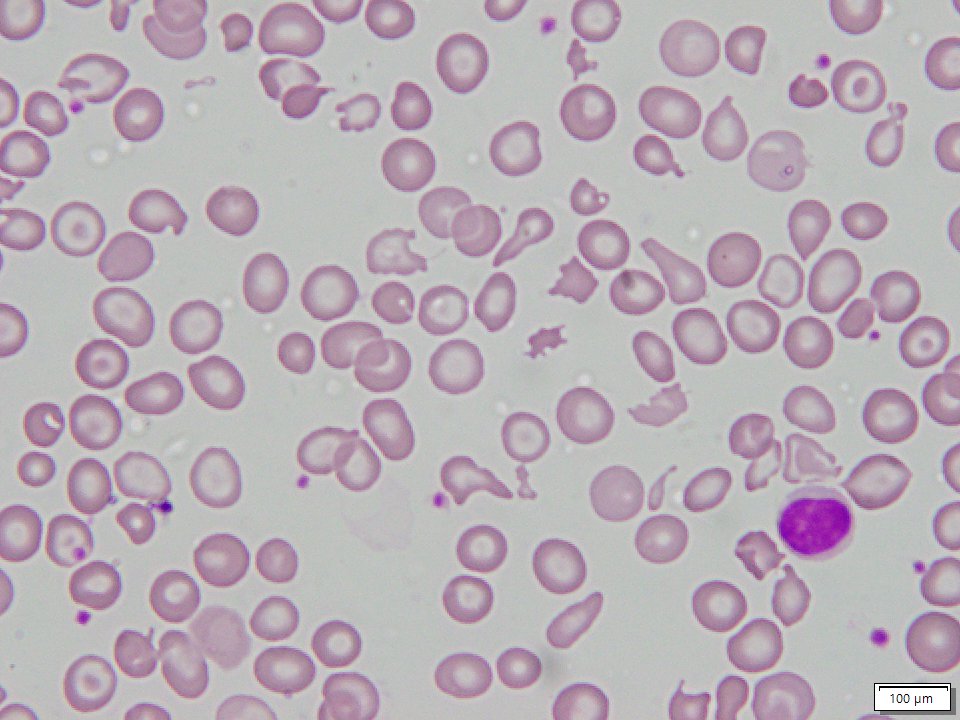
Hb E/β-thalassaemia results from co-inheritance of a β-thalassaemia allele from one parent and the structural variant Haemoglobin E from the other. Haemoglobin E results from a G→A substitution in codon # 26 of the β globin gene, which produces a structurally abnormal haemoglobin as well as activates a cryptic splice site, resulting in abnormal messenger RNA (mRNA) processing. The level of normally spliced mRNA, βE, is reduced30 and, because a new stop codon is generated, the abnormally spliced mRNA is non functional. Hence, haemoglobin E is synthesized at a reduced rate, and behaves like a mild form of β-thalassaemia. The pathophysiology of Hb E/β-thalassaemia is related to many factors including reduced β chain synthesis resulting in globin chain imbalance, ineffective erythropoiesis, apoptosis, oxidative damage and shortened red cell survival31,32. In general, it appears that the recognized instability of haemoglobin E is a minor factor in the overall pathophysiology of Hb E/β-thalassaemia, except during intercurrent febrile illnesses during which such instability may result in accelerated haemolysis33.
The reasons for the extraordinary clinical heterogeneity of Hb E/β-thalassaemia are not completely understood. The condition may present as a mild and asymptomatic anaemia, or as a life-threatening disorder requiring transfusions from infancy. In a clinic-based population in Sri Lanka, many fewer cases of Hb E/β-thalassaemia were observed than would be expected based on the Hardy-Weinberg equation, probably reflecting the mildness and variable clinical course of some cases of Hb E/β-thalassaemia3.
As well, the phenotype of Hb E/β-thalassaemia may be unstable. A modified “natural history” study of Hb E/β-thalassaemia in children in Sri Lanka highlighted the instability of phenotype over the first ten years of life, during which there was a variable, and changing, pattern of anaemia and erythroid expansion. In many patients, the phenotype became more stable later in development, and it was frequently possible to stop blood transfusion in a proportion of older patients with no apparent subsequent effects on activities of daily living, or quality of life24. Conversely, it is worth noting that while little is documented about the clinical course of older patients, the limited data available indicate that many adults appear to develop worsening anaemia with age. The lack of a standardized, robust classification of disease severity is a major impairment in understanding the clinical spectrum of Hb E/β-thalassaemia and how it may change with age.
Another important finding identified in the modified “natural history” study of Hb E/β-thalassaemia in Sri Lanka was that in these patients, considerable phenotypic heterogeneity occurred within a relatively narrow range of haemoglobin values. The mean difference in haemoglobin concentration between the mildest and most severe groups was only approximately 1 to 2 g/dl. In patients who had been maintained on regular or “on demand” transfusions, pre-transfusion steady-state haemoglobin concentrations (mean 7.0 g/dl) were not clinically very different (mean 6.1 g/dl) from those in patients who had never been initiated on regular transfusions24.
Clinical severity categories of haemoglobin E/β-thalassaemia
Attempts to categorize the severity of Hb E/β-thalassaemia have included the assignment of patients to “severe” and “mild” disease groups, between which putative genetic and environmental factors are then compared24,34. In Sri Lanka, Premawardhena et al24 classified 109 patients (aged one to 51 years) into five classes of severity ranging from very mild to very severely affected patients. About a quarter of the patients were transfusion-independent while the remainder were maintained on either regular or intermittent (on demand) transfusion. In many patients, clear information as to why or whether transfusions had been necessary was lacking24,35,36. Group 1 included those patients who had undergone only minimal transfusion and had normal growth and sexual maturity; Group 1 children had adequate growth and all patients rated quality of life as exceeding 5 on the 10-point scale. Group 2 comprised patients similar to those in group 1, except for transfusion history: these patients had a longer history of transfusions. Group 3 included patients who had undergone splenectomy with a beneficial response and during the two years following splenectomy an improvement in quality of life and increase in height velocity were observed. Group 4 included those patients who, while maintained off transfusions, were struggling as evidenced by poor growth, delayed sexual maturation, and marginal self-reported quality of life (less than 5 on the 10-point scale). Group 5 comprised those patients who, because of problems similar to those observed in group 4 patients, were unable to function off transfusions.
Factors that influence clinical severity
There is an emerging understanding of the genetic and environmental factors that influence the clinical course and severity of anaemia in Hb E/β-thalassaemia. Genetic factors include the type of β-thalassaemia mutation co-inherited with Hb E, the co-inheritance of alpha (α) thalassaemia, and that of polymorphisms shown to be associated with increased synthesis of foetal haemoglobin.
Inheritance of the beta thalassaemia allele trans to haemoglobin E: In early studies, Thai investigators27 suggested that patients who co-inherit a mild β-thalassaemia allele with Hb E may have disease on the mild end of the spectrum, while those who co-inherited severe β+ or β°-thalassaemia alleles might be more severely affected. However, a less severe β-thalassaemia mutation may be only one of several genetic modifiers. Winichagoon et al27 defined the mutations in 90 Thai patients with steady-state haemoglobin concentrations varying from 4.2 to 12.6 g/dl, the same severe β-thalassaemia mutation was observed in both mild and severely anaemic patients. In the 36 patients identified as having a “milder” clinical phenotype, nearly half (42%) co-inherited a modifying mutation other than a mild beta-thalassaemia allele, including the XmnI polymorphism, α+ thalassaemia or haemoglobin H-Constant Spring. More recent studies confirm the severity of the β mutation may be an important but not consistent influence on the clinical diversity of Hb E/β-thalassaemia24,26,37. In another study of the Thai population conducted in 2000, a mild Hb E/β-thalassaemia phenotype, considered to be related to the interaction between Hb E and the mutation at nucleotide –28 in the ATA box of the β globin gene, was reported in 6 of 88 patients26. In other mildly affected patients, however, the β-thalassaemia mutation was one not known to be associated with mild disease. Studies in other populations, including from India and Sri Lanka, suggest that β-thalassaemia mutation has an influence somewhat more limited than previously believed on the clinical severity of Hb E/β-thalassaemia24,37.
In summary, the β-thalassaemia allele in trans to Haemoglobin E does not seem to account for the wide phenotypic variation observed in Hb E/β-thalassaemia and clearly other modifying genetic factors must be considered26.
Alpha-thalassaemia: Patients with Hb E/β-thalassaemia who co-inherit a determinant for α-thalassaemia should in theory, have a reduced number of unmatched α globin chains, which would be expected to lead to more balanced globin chain synthesis and a milder phenotype. Early studies suggested that Hb E/β-thalassaemia patients with an α+thalassaemia allele demonstrated, on average, higher steady-state haemoglobin concentrations than those without α-thalassaemia26,38. Recent studies supporting the beneficial effect of α-thalassaemia on Hb E/β-thalassaemia also indicate that, as with the beta globin gene mutation, the influence of this factor on the clinical severity of Hb E/β-thalassaemia may not be altogether straightforward. The effect of the co-inheritance of different copy numbers of the α globin genes was analyzed in over 900 Thai Hb E/β-thalassaemia patients, aged 2 to 77 yr, who demonstrated a wide range of steady-state haemoglobin levels (3.2-12.1 g/dl). A total of 8.8 per cent patients of this group were demonstrated to have a form of α-thalassaemia; most often identified was a form of deletional a+thalassaemia [–α3.7/αα (n=51); –α4.2/αα (n=8)] while the arrangement –α3.7/–α3.7was identified in only one patient39. The mean age at presentation of patients with α thalassaemia (10.4 ± 9.2 yr) was more than that in those without α-thalassaemia (3.7 ± 5.5 yr). Moreover, while about a third (32%) of patients with a normal α-globin gene arrangement required regular blood transfusions, none with α-thalassaemia required regular transfusions, although several had received one or more transfusions during intercurrent illnesses. Within the longitudinal study of patients in Sri Lanka24, the restriction of α+thalassaemia alleles to the two groups with the mildest phenotypes suggested that α-thalassaemia has a substantial ameliorating effect on the severity of Hb E/β-thalassaemia. In a group of Indian patients with Hb E/β-thalassaemia, those co-inheriting α-thalassaemia also generally presented with a mild phenotype, while patients with triplicated alpha genes were reported to have a more severe phenotype in which frequent transfusions were often required40.
Co-inheritance of α-thalassaemia appears to be a major genetic factor modifying clinical phenotype, including the finding that a considerable number of patients who co-inherit α-thalassaemia may be diagnosed later in life. Clearly, while mild Hb E/β-thalassaemia may occur in the absence of α thalassaemia, the presence of α-thalassaemia genes should always be considered in mild cases of Hb E/β-thalassaemia.
Determinants associated with increased haemoglobin F synthesis: Several studies provide evidence that polymorphisms associated with increased synthesis of foetal haemoglobin, including the presence of the G to T substitution -158 5’ to the Gg gene (the Xmn1 polymorphism), the presence of a single-nucleotide polymorphism in the gene BCL11A, and other genetic loci, may be associated with increased synthesis of foetal haemoglobin, and with a milder clinical phenotype in Hb E/β-thalassaemia.
The XmnI polymorphism appears to be an important modifying factor in haemoglobin F synthesis. In Chinese heterozygotes for β-thalassaemia as well as in healthy Europeans, the Xmn1 polymorphism has been reported to account for approximately 9 to 13 per cent of the genetic variance of haemoglobin F41–43. Thai patients with Hb E/β-thalassaemia and a Xmn1 +/+ genotype27 had higher total haemoglobin (8.5 compared to <7.0 g/dl) and higher foetal haemoglobin concentrations than those with a XmnI -/- genotype. These findings are consistent with previous findings suggesting that homozygosity for the Xmn1 polymorphism may be necessary to ameliorate the severity of thalassaemia. In the longitudinal study of Hb E/β-thalassaemia in Sri Lanka, a positive correlation between concentrations of haemoglobin and foetal haemoglobin, and homozygosity for the Xmn1 polymorphism was reported24. Patients with the Xmn1 +/+ genotype were identified only in mildly affected patients; conversely, patients with “severe” phenotypes, including a history of early presentation to medical attention, were more likely to have Xmn1 -/-. Other studies confirm that patients with the arrangement of Xmn1 -/- presented at a younger age, and were more likely to receive transfusions, compared to those with an arrangement of Xmn1 (+/-)37. Other investigators44 who compared the presence of single nucleotide polymorphisms (SNPs) within the locus control region of the β globin gene cluster and the δ gene with clinical severity confirmed that the most robust predictor for a mild clinical phenotype was the Xmn1 polymorphism. While some conflicting data have been presented, overall, homozygosity for the Xmn1 polymorphism appears to be an important factor modifying the severity of Hb E/β-thalassaemia45.
Additional genetic factors which modify disease severity await discovery. Association studies to elucidate the role of genetic polymorphisms known to influence globin gene expression and erythropoiesis, which may contribute to the variable clinical severity of Hb E/β-thalassaemia are underway. Recently, six SNPs in the BCL11A gene on chromosome 2p16.1 were reported to be associated with F-cell numbers in a study of 179 unrelated normal subjects from a British twin registry41 and with foetal haemoglobin levels among Sardinians with β-thalassaemia. Quantitative trait loci (QTL) associated with increased foetal haemoglobin synthesis have been described on chromosomes 6q23, 8q, and Xp2246–48. The contribution of the QTL on chromosome 6q23 to the genetic variance of haemoglobin F/F-cells is estimated to be 19 per cent, and the contribution of BCL11A to be 15 per cent41–43. Sedgewick et al49 reported that SNPs in BCL11A are associated with foetal haemoglobin production in Thais with either β-thalassaemia or Hb E trait (as well as in African Americans with sickle cell anaemia), and with F-cell numbers in Chinese individuals with β-thalassaemia trait. These limited studies suggest that BCL11a polymorphisms may be important modulators of foetal haemoglobin in HbE/β-thalassaemia. Sripichai and colleagues50 analyzed 1060 Hb E/β-thalassaemia patients for 22 SNPs within seven genes known to influence globin gene expression, and erythropoiesis, including β-protein 1, erythropoietin, and transcription factors EKLF, GATA-1, and NF-E2. No statistically significant differences between mild and severe phenotypes were observed for polymorphisms in the candidate genes. A later genome-wide association study conducted in 618 patients with Hb E/β-thalassaemia51 analyzed 23 SNPs in three independent genes/regions identified as being significantly associated with disease severity. The strongest association was observed with SNPs in the β globin gene cluster (chr.11p15); rs2071348 of the HBBP1 gene followed by the association with SNPs identified in the intergenic region between the HBS1L and MYB genes (chr.6q23). A third potentially important region was located in the BCL11A gene. These findings have been replicated in a cohort of 174 Indonesian patients45. These data suggest that several genetic loci act in concert to influence foetal haemoglobin levels of Hb E/β-thalassaemia patients, with three reported loci and the alpha globin gene locus identified as predictors of disease severity52.
Other investigators53 reported an association of the HBS1L-SNP7 polymorphism in exon 1 of the beta globin gene with haemoglobin F levels in 30 patients selected for mild and severe phenotypes of Hb E/β-thalassaemia, different levels of foetal haemoglobin, and different XmnI polymorphisms. Genotyping of a C32T polymorphism identified in a potential E-box binding site of HBS1L in exon 1 was carried out in 455 patients with Hb E/β-thalassaemia. HBS1L-SNP7 had a slight, but statistically significant, effect in modulating absolute foetal haemoglobin levels among patients with Hb E/β-thalassaemia and Xmn1 -/-, while the effect of HBS1L-SNP7 was more pronounced among patients with Xmn1 +/-. The overall conclusion was that this polymorphism is of minor effect in comparison with the influence of Xmn1.
Other Modifying Factors
α-haemoglobin stabilizing protein (AHSP) gene: The α-haemoglobin stabilizing protein (AHSP), a chaperone of α-globin, has been suggested as another genetic modifier of severity in thalassaemia54. AHSP was not observed to be a modifying factor of the clinical severity of β-thalassaemia in Thai patients55 or in patients with Hb E/β-thalassaemia in Sri Lanka24; but has been confirmed by others50.
Bilirubin metabolism: Chronic hyperbilirubinaemia, gallstone formation, and gall bladder disease may significantly worsen the phenotype of patients with Hb E/?-thalassaemiaβ-thalassaemia. There is now clear evidence that the inherited variability in the function of the gene for UDP-glucuronosyltransferase-1 (UGT1*1, the enzyme responsible for hepatic glucuronidation of bilirubin) underlies the chronic hyperbilirubinaemia of Gilbert’s syndrome56, some cases of thalassaemia trait57, and some of the variations in the frequency of gallstones in patients with hereditary spherocytosis58. The increased level of bilirubin in these disorders has been related to a polymorphism of the promoter of the UGT1*1 gene. Premawardhena et al59 have reported that the UGT*1 genotype is important in the genesis of gallstones in patients with Hb E/β-thalassaemia. These investigators found significantly higher bilirubin levels in patients with Hb E/β-thalassaemia and the 7/7 genotype of the UGTA1A promoter, compared with those with 6/6 and 6/7 genotypes. Patients with the 7/7 genotype were also reported to be more likely to develop gallstones over the age of 15 yr.
Co-inheritance of other haematologic disorders: Co-inheritance of other haematologic abnormalities may contribute to the variation in phenotype in patients with Hb E/β-thalassaemia. A family in which the interaction between pyrimidine-5 nucleotidase-I (P5N-I) deficiency and homozygous Hb E resulted in severe haemolytic anaemia, has been reported60. This individual was demonstrated to have a mutation in the P5N-1 gene61 affecting expression of the P5N-1 enzyme, believed to be susceptible to free radical damage. While P5N-I deficiency typically presents as mild haemolytic anaemia, in this patient haemolysis was more severe than would be expected in either condition alone. This raises a possibility that coincidental inhibition of P5N-I activity may contribute to the severe haemolysis associated with some unstable haemoglobin variants, including Hb E.
Variation in iron loading: A common dilemma often encountered in the clinical setting is whether the poor growth and delayed sexual maturation observed in many patients with Hb E/β-thalassaemia is a result of chronic anaemia, iron overload, or a combination of these factors. As reported in a study in which precise measurements of iron loading were determined systematically, many patients with a clinical history of a few transfusions had substantial iron burdens and evidence of end-organ damage not evident by screening tests62. Although previous studies described the common haemochromatosis alleles in Asian patients to be rare63–65, Lok et al66 have reported some novel mutations in haemojuvelin, hepcidin, and mutations in the SLC40A1 gene, which encodes for ferroportin, in Asian patients from countries not normally associated with haemochromatosis. These mutations resulted in different presentations of iron overload, suggesting that primary iron overload may not be as rare as was previously considered in these geographic areas. Studies to determine the rates and severity of gastrointestinal iron loading in Asia, as well as the effect of variability in iron loading on phenotype of Hb E/β-thalassaemia, are awaited.
Hb E/β-thalassaemia is characterized by different clinical manifestations at particular stages of development. Whether this reflects developmental changes in adaptation to anaemia, or other mechanisms, is presently unclear. In Sri Lankan patients with Hb E/β-thalassaemia, serum erythropoietin (EPO) concentrations assayed over five or more years of observation were significantly correlated with steady-state haemoglobin concentrations, while a significant decline in increases in serum EPO in the presence of anaemia was observed with advancing age24. Extended studies confirmed an attenuated increase in EPO in association with haemoglobin concentration with advancing age67. The effect of age on an attenuated increase in EPO was independent of haemoglobin concentration. In a group of children with mild phenotypes, there was a very modest increase in EPO in the presence of anaemia compared with that observed in the entire cohort. Although genetic modifiers that influence the severity of the phenotype in many of these children had been identified, the reason for milder disease in others was not clear. The possibility that mild disease could be related to inherent differences in EPO response remains to be determined.
In other patients, the effect of high levels of EPO on steady-state haemoglobins was limited: high levels of EPO production in thalassaemia may result in considerable expansion of the erythroid mass68, but this erythropoiesis in severe thalassaemia is, largely, ineffective. Hence, the consequences of high levels of EPO includes many disease complications including hepatosplenomegaly and bone deformity with less influence on steady-state haemoglobin concentrations. This was suggested by the observation that the rate of splenic enlargement, one of the consequences of high levels of EPO production in thalassaemia, appeared to vary in younger and older patients69. In older Sri Lankan patients, the spleen enlarged slowly over time, while over the same period in younger patients with steady-state haemoglobin concentrations in a range similar to that of the older patients, more rapid splenic enlargement was reported69.
These findings, if confirmed, appear to suggest that developmental changes in EPO responsiveness to severe anaemia may have important implications for the clinical management of Hb E/β-thalassaemia. A exuberant EPO response to anaemia in early childhood, and a decline in EPO response with age, may be in part responsible for some of the phenotypic instability observed in Hb E/β-thalassaemia during early childhood24. If the increase in serum EPO in response to a particular haemoglobin level declines with age, drive to erythroid expansion might in parallel also decline. If, over early childhood during the period of maximum potential EPO response to anaemia, the magnitude of this response could be partly suppressed by transfusions, certain complications of erythroid expansion might be avoidable. It follows, then, that it may be possible to reduce the frequency or stop transfusions in some patients as the serum EPO response to a particular haemoglobin concentration declines with age. Indeed, in some patients reported by Premawardhena et al24 it was possible to stop regular transfusions after the age of 9-10 yr without apparent deleterious effects. They proposed that a programme of “transient transfusion” may reduce complications related to iron overload, as well save medical resources in the emerging countries in which Hb E/β-thalassaemia is common. These findings await confirmation in other populations. In the two previous reports of EPO response to anaemia in Hb E/β-thalassaemia70,71, one reported a difference in an overall pattern of response between children and adults which did not reach statistical significance71. In another study of patients with sickle cell anaemia, 10 adults appeared to show a less robust increase in serum EPO than those of children at approximately the same steady-state haemoglobin concentration72. Although there have been no extensive studies of EPO response at different age groups in patients with Hb E/β-thalassaemia and profound anaemia, longitudinal analysis of individuals with milder forms of anaemia due to several other causes have yielded inconsistent findings. In some studies, there has been a less robust increase in serum EPO to anaemia in older patients, while in others, the response appeared to be similar across the age range73–75.
Environmental influences on the phenotype of Hb E/β-thalassaemia
Malaria: There is a high frequency of malaria, both Plasmodium falciparum and P. vivax, throughout most of the continent of Asia. Although P. vivax was previously considered to be a relatively mild disorder, this has recently emerged as a serious public health problem in many Asian countries76,77. In Sri Lankan patients with Hb E/β-thalassaemia, a high proportion was shown to be positive for antibodies to P. vivax and P. falciparum, although with its excellent public health progammes, transmission rates for both forms of malaria have dropped dramatically over recent years in this country. Among the younger patients, 28 per cent were positive for P. vivax using DNA analysis, a sensitive diagnostic tool in regions of low transmission68. Follow up studies including age-matched controls reported a significantly higher level of malarial antibodies, particularly to P. vivax in young children, in patients with Hb E/β-thalassaemia compared with the control population. There was a highly significant difference in levels of malarial antibodies in splenectomized patients with Hb E/β-thalassaemia, compared with those with intact spleens. However, antibody levels in patients with Hb E/β-thalassaemia and intact spleens were still significantly higher compared to those the control population. It is possible that, given that P. vivax is known to preferentially invade young red cells, children with a young red cell population arising from ongoing haemolysis and reticulocytosis in Hb E/β-thalassaemia, may be susceptible to infection with P. vivax. If these findings are confirmed through other parts of Asia, patients with Hb E/β-thalassaemia should be provided prophylaxis against both forms of malaria. Similar studies need to be carried out, especially in parts of India and other regions with a high transmission rate of P. vivax.
Management and Future
Studies throughout Asia, particularly in the cohort of Sri Lankan patients carefully observed over more than a decade, have noted the ability of many patients with Hb E/β-thalassaemia to adapt to haemoglobin steady-state concentrations that would not be as well tolerated in other beta-haemoglobinopathies. In fact, the evidence suggests that the steady-state haemoglobin concentration, per se, may be of limited value in deciding in which patients with Hb E/β-thalassaemia regular transfusions are indicated.
It is now generally appreciated that no patient with Hb E/β-thalassaemia should be placed on a regimen of regular transfusions without an extended period (of at least 3-6 months without intercurrent illness) in which growth, pubertal development if applicable, quality of life, symptoms and signs of anaemia including changes in spleen size, are monitored. By contrast, the age of presentation to medical attention, homozygosity for the Xmn1 polymorphism, and co-existent α-thalassaemia appear to be valuable prognostic indicators.
Several important questions remain. While some explanations are now available for the phenotypic heterogeneity of Hb E/β-thalassaemia, including the better-defined influence of certain genetic factors as possible modifiers, cross-sectional studies of different ages suffer from several difficulties. In particular, in Hb E/β-thalassaemia because of changing phenotypes and variable medical interventions, it is difficult to accurately characterize the severity of this disease. Its remarkable phenotypic diversity is still not well understood. Such understanding would be augmented by a cohort study from birth or, because a significant proportion of patients with this condition present later than the first year of life, in a study to define phenotypes in children before the age of 12 yr and prior to substantial medical intervention.
Given what we have learned, what is the optimal management of patients with Hb E/β-thalassaemia who fail to adapt to anaemia? Although in one study24 evidence for benefit on growth and development following splenectomy was presented, it is unclear whether the frequent use of splenectomy is acceptable. It is clear that morbidity and mortality due to infection at all ages was significantly higher in splenectomized patients. But, because it now appears that marrow expansion and increasing splenomegaly are less marked in older patients, a trial or observational study of transient transfusion during the period of major expansion appears justified.
It will also be important to establish the reasons for variable iron loading, and the problems of patients who experience poor growth and sexual retardation in the absence of severe iron loading in larger cohorts with Hb E/β-thalassaemia. Further exploration of individual responses to anaemia is also required. There also remain limited data on the environmental factors which may modify the course of this disease; infection with malaria, for example, may prove an important modifying factor.
Finally, it is clear that the costs of thalassaemia care will represent an important proportion of the future healthcare budgets of Asia78. Hence, consideration of general guidelines for management, including careful consideration of maintaining such patients off transfusions, have been suggested for the management of Hb E/β-thalassaemia.